Gastric Reflux Surgery
Gastro Esophageal Reflux Disease(GERD)
An Overview GERD (GASTRO ESOPHAGEAL REFLUX DISEASE)
All of us have experienced gastro intestinal symptoms like acidity, indigestion, heart burns / GERD, bloating, diarrhoea, gas, stomach pain, cramps, constipation etc. At CALOMS, we provide with best medical, diagnostic, surgical care for GERD.
If you have recurrent heartburn or acid reflux or ‘acidity’ twice a week or more, you may have GERD (Gastro Esophageal Reflux Disease). While acid medicines give symptomatic relief from pain of acid reflux and heartburn, it doesn’t restore the natural anatomy and generally doesn’t stop the disease progression. Acid reflux and heartburn medications just mask the problem usually causing more and more medication to be needed with less relief.
There is no need to continue to suffer with heartburn and acid reflux. At CALOMS we specialise in treating acid reflux disease and GERD(Gastro Esophageal Reflux Disease) and is one of the best centers in Pune, India to be trained and providing the most recent treatment options for GERD.
At CALOMS we offer the best treatment options including scientifically approved surgical treatment – Laparoscopic Nissens Fundoplication and Hiatus Hernia repair for chronic gastro esophageal reflux disease. Dr Girish Bapat specialises in the laparoscopic treatment and offers most advanced treatment.

What Is Gastro Esophageal Reflux Disease (GERD)?
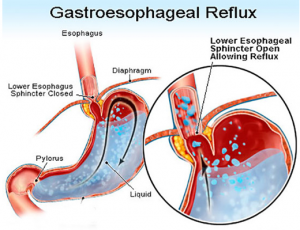
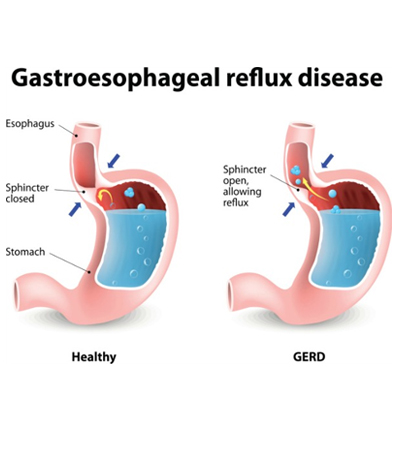
Oesophagus or food pipe carries food from our mouth to our stomach. At the lower end of oesophagus there is a valve which opens to allow the food to pass through. The valve will then close in order to prevent the stomach contents to leak back or reflux into the Oesophagus. Therefore it is supposed to maintain a ‘one way traffic’.
People who are suffering with Gastro Oesophageal reflux disease, GERD or acid reflux disease have problems with this lower oesophageal or gastro oesophageal valve not closing properly causing acid to reflux or leak into the oesophagus ‘leaky valve’.
Lining of oesophagus (food pipe) is very delicate, when refluxed stomach acid touches the lining of the oesophagus, it causes a burning sensation in the chest or throat called heartburn. The distal oesophagus is adapted for some degree of reflux. However, significant reflux may lead to troublesome symptoms and complications.
GERD (Gastric reflux) is very common and ranges widely in severity. It is estimated that between 25% – 50% of adults in experience some degree of reflux, and 5 – 10 % experience daily symptoms. GERD is 2-3 times more common in men than women.
Symptoms of Gastro Esophageal Reflux Disease (GERD)
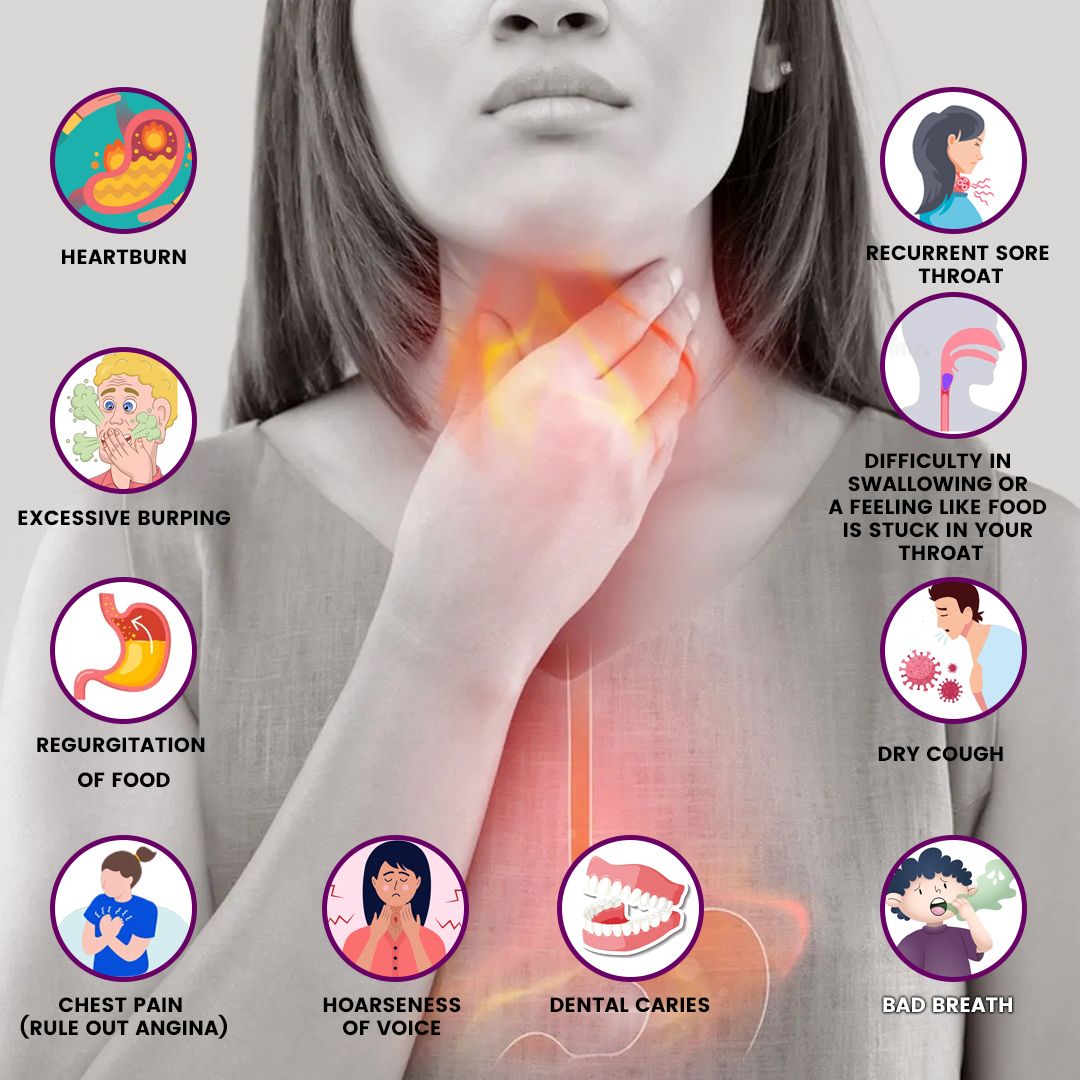
Though majority of patients with GERD (Gastric reflux) complain of persistent heartburn and/or acid regurgitation, patients may experience symptoms of GERD in a variety of ways. Symptoms of GERD may include:
- Heartburn
- Excessive burping
- Regurgitation of food
- Chest pain (rule out angina)
- Hoarseness of voice
- Recurrent sore throat
- Difficulty in swallowing or a feeling like food is stuck in your throat
- Dry cough
- Bad breath
- Dental caries
Causes of Gastro Oesophageal Reflux Disease:
It’s thought that GERD is caused by a combination of factors, but the most common is the failure of the lower oesophageal sphincter (LOS) – a ring of muscle towards the bottom of the oesophagus which acts like a one way valve.
In GERD, this sphincter doesn’t close properly, allowing acid to leak up into the oesophagus.
A number of conditions can predispose to GERD
- Pregnancy
- Obesity
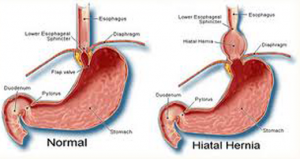
- Presence of a hiatus hernia
- Delayed gastric emptying or esophageal dysmotility
- Connective-tissue disorder such as scleroderma
Factors that can aggravate GERD symptoms.
- Smoking or tobacco chewing
- Alcohol intake , excessive tea/ coffee
- Eating large meals or eating late at night or skipping meals
- Eating oily, spicy and acidic foods
- Drinking aerated drinks like coca cola, pepsi, beer
- Taking pain killers like brufen, voveran
Complications of Gastro Esophageal Reflux Disease:
Apart from poor quality of life, GERD (Gastric reflux) can disrupt sleep, work and prevent patients from enjoying food and socialising. Chronic gastric acid reflux can lead to potentially serious complications:
- Oesophagitis (Inflammation, irritation, or swelling of the esophagus)
- Stricture (Narrowing of the esophagus)
- Barrett’s Oesophagus can potentially become cancer.
- Damage to teeth and enamel from recurrent acid exposure
Oesophagitis (Inflammation, irritation, or swelling of the esophagus)
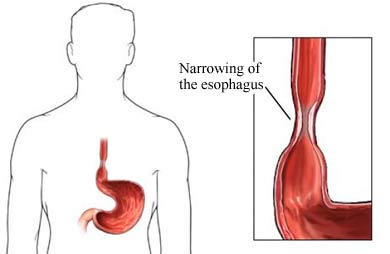
Stricture (Narrowing of the esophagus)
Barrett’s Oesophagus can potentially become cancer.

Damage to teeth and enamel from recurrent acid exposure
Diagnosis
Your doctor may be able to diagnose GERD based on frequent heartburn and other symptoms
Further testing is required to confirm or disprove the diagnosis of GERD, while checking for any other possible causes of your symptoms, such as functional dyspepsia (irritation of the stomach or food pipe) or achlasia.
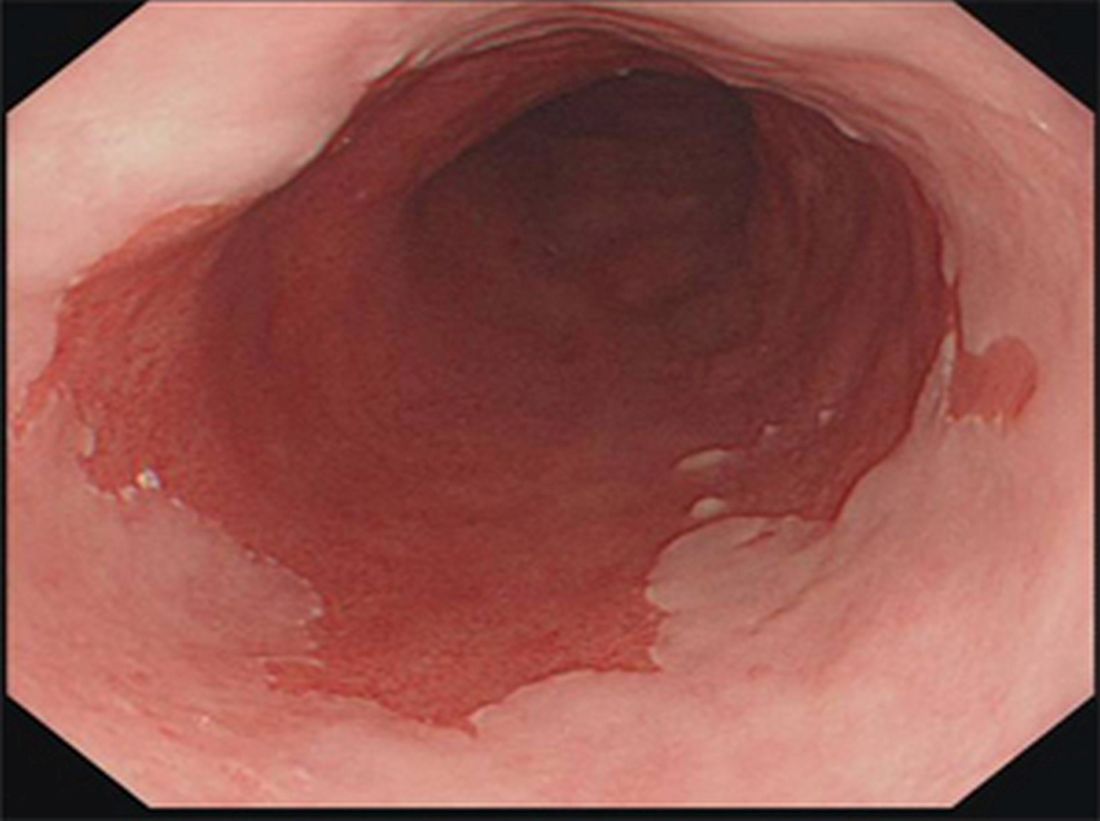
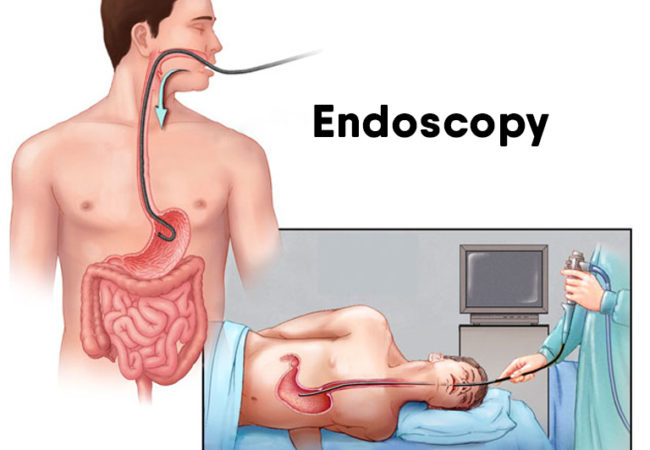
Endoscopy
- Endoscopy demonstrates anatomy and identifies the possible presence and severity of complications of reflux disease (oesophagitis, Barrett oesophagus, strictures (narrowing)).
- Biopsy samples of suspicious lesions can be obtained during endoscopy.
- Endoscopy also excludes the presence of other diseases like peptic ulcer, achlasia and stomach cancer that can present similarly to GERD.
- The endoscopist should also make a note of the presence of a hiatus hernia which helps in planning further treatment including surgery.
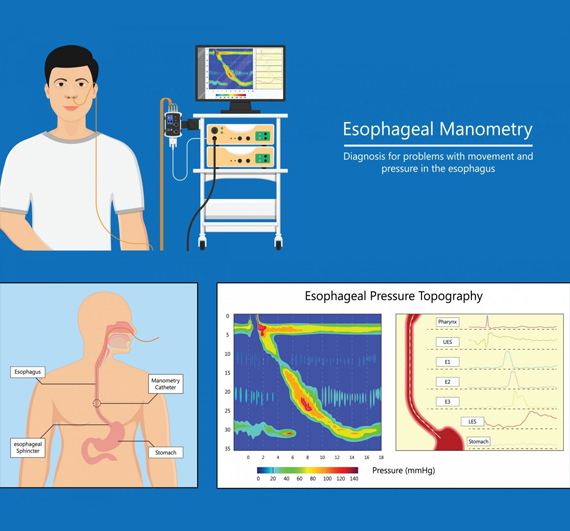
Manometry
This specialised test used to assess the function of the oesophagus (food pipe) and Lower Oesophageal Sphincter (LOS)
- High-resolution oesophageal manometry is done using a 32-channel flexible catheter with pressure-sensing devices arranged at 1-cm intervals, placed into the food pipe through the nose
- The study is conducted in approximately 15 minutes, during which time the patient performs 10 swallows. A colour plot is generated and shows the response of the upper oesophageal sphincter and LOS as well as of the oesophageal body.
- Oesophageal manometery provides information on peristaltic and non-peristaltic activity of the oesophagus as well as the resting pressures of the upper and lower oesophageal sphincters
- Oesophageal manometry can exclude motility disorders such as achalasia and it identifies patients with ineffective esophageal body peristalsis. It is important to note that repeated exposure of the esophagus to gastric reflux can in itself lead to esophageal dysmotility
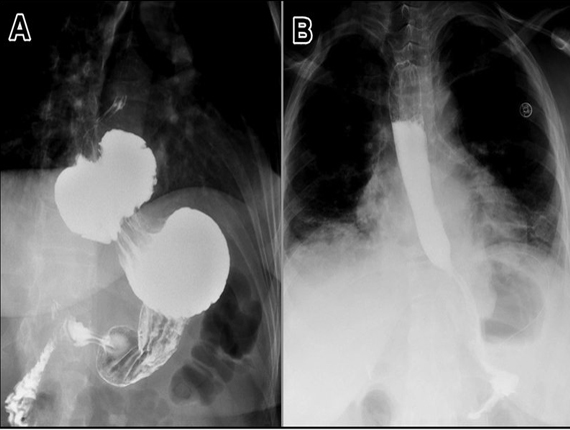
Barium Studies
This is a specialised X-ray of your food pipe (oesophagus), stomach and upper small intestine (duodenum). Sometimes called a barium swallow or upper GI series, this procedure involves drinking a chalky liquid that coats and fills the inside lining of your digestive tract. Then X-rays are taken of your upper digestive tract. The coating allows your doctor to see a images of your oesophagus, stomach and upper intestine (duodenum). It also helps to diagnose presence of hiatus hernia.
It is also used to exclude delayed gastric emptying as the main cause for reflux . Additional conditions that can be identified on barium study are: oesophageal webs, rings, diverticula and strictures, as well as functional motility abnormalities such as achalasia and diffuse oesophageal spasms
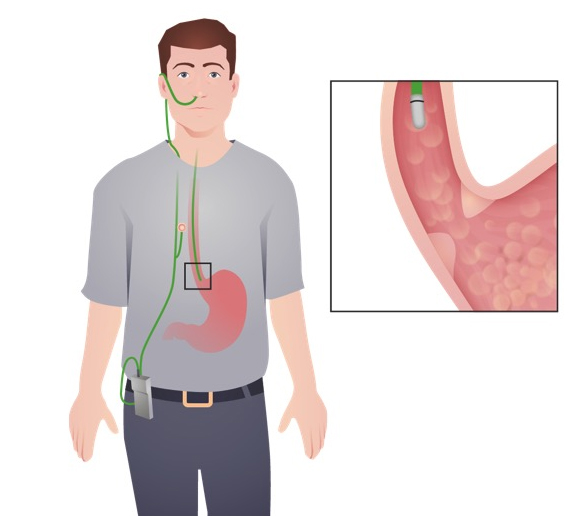
Ambulatory pH study with intraluminal impedance
- 24-hour pH monitoring is the gold-standard investigative modality for pathological reflux and it is conducted with a thin catheter that is passed down the oesophagus through the patient’s nose.
- It is performed off of acid-suppression therapy for 1 week
- This test is done to monitor the amount of acid in your oesophagus.Ambulatory acid (pH) probe tests use a device to measure acid for 24 hours.
- The device identifies when, and for how long, stomach acid regurgitates into your oesophagus.
- It records reflux symptoms as they occur and correlates these with patient symptoms as an event marker
An alternative to the 24-hour pH study is the BRAVO study, a wireless capsule that negates the use of a nasogastric catheter that some patients are not able to tolerate, and it also captures data over a longer (48 hour) period
Treatment of Gastro- Oesophageal reflux disease (GERD)
Treatment of gastroesophageal reflux disease (GERD) involves a stepwise approach. The goals are to control symptoms, to heal oesophagitis, and to prevent recurrent oesophagitis or other complications. The treatment is based on :
(1) lifestyle modification and
(2) control of gastric acid secretion through medical therapy with antacids or PPIs or
(3) surgical treatment with corrective antireflux surgery.
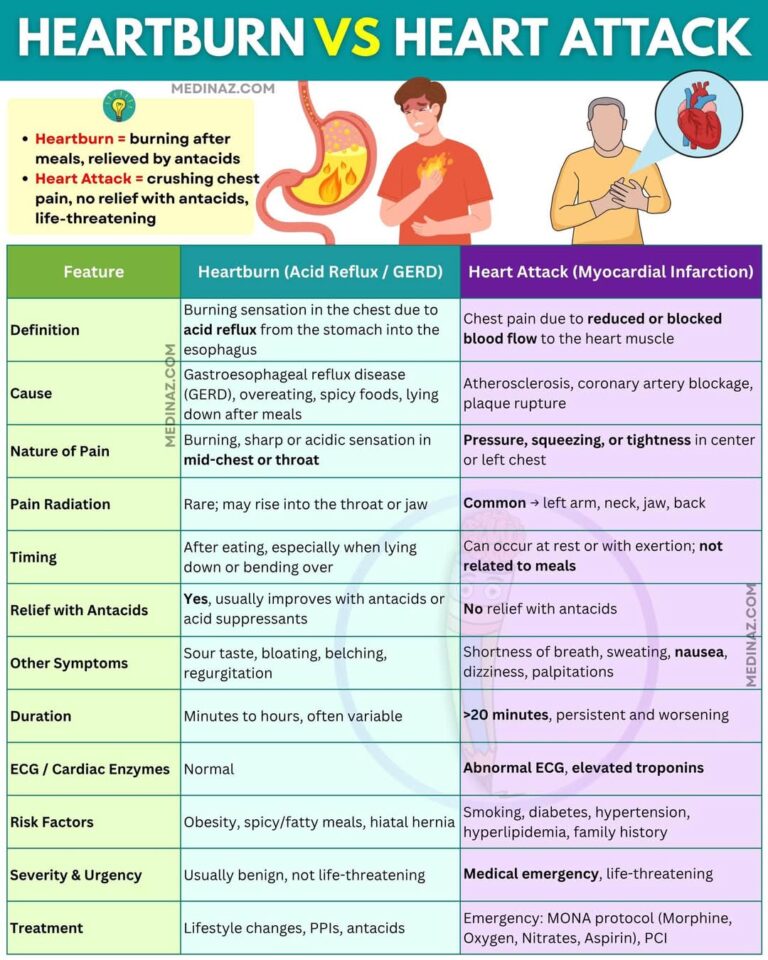
Heartburn Vs Heart Attack
Lifestyle modification
If you have GERD, you may find the following self-care techniques useful:
- If you’re overweight, losing weight may reduce your symptoms, as it will reduce pressure on your stomach.
- Giving up smoking/ tobacco
- Eating smaller, more frequent meals, rather than large meals can help.
- Plenty of fresh fruits, salads and water
- Make sure you have your evening meal three or four hours before bedtime.
- Alcohol, coffee, chocolate, tomatoes, or fatty or spicy food can trigger the symptoms of GERD.
- Raise the head of your bed by around 20cm (8 inches) by placing a piece of wood or brick under it. This may improve your symptoms. Don’t use extra pillows, because it may increase pressure on your abdomen.

Medication
-
- Headaches
- Diarrhoea
- Nausea
- Abdominal pain
- Constipation
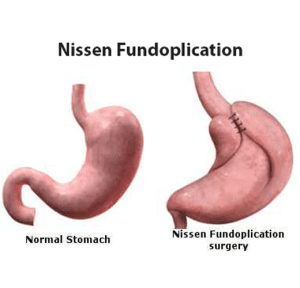
Surgery- Laparoscopic Fundoplication and Hiatus Hernia Repair
What is laparoscopic fundoplication and Hiatus Hernia Repair?
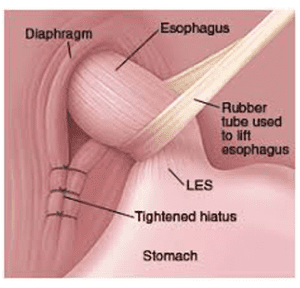
Laparoscopic fundoplication is a keyhole operation which is performed for patients with severe acid reflux that no longer responds to anti-acid medications and life-style adaptive changes. This operation is also performed in patients with symptomatic hiatus hernias (hernias where part of the stomach slips through an abnormally widened opening in the diaphragm). A hiatus hernia may make acid reflux more likely. A hiatus hernia may occur without reflux, and reflux may occur without a hiatus hernia. Commonly however, these two do co-exist and when surgery is needed, they are usually treated together.
What does Operation involve?
The aim of the fundoplication operation is to prevent acid from the stomach refluxing into the oesophagus (food pipe). The procedure involves
(1) Repositioning any portion of stomach that has herniated into the chest (hiatus hernia) back into the abdomen,
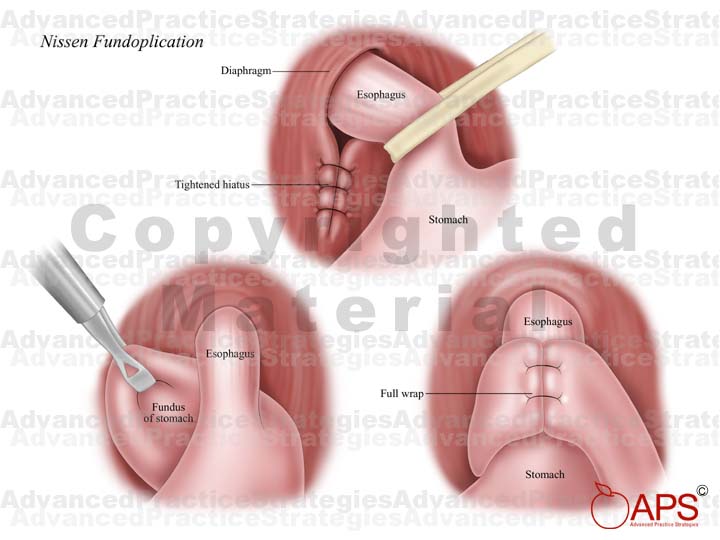
(2) Narrowing the opening in the diaphragm through which the oesophagus (food pipe) passes into the abdomen and
(3) wrapping the upper part of the stomach around the lower oesophagus (the wrap) to create a valve at the lower end of the oesophagus (gullet). The wrap itself may be complete or partial depending on patient factors, severity of reflux etc. The operation is performed by Laparoscopy and takes about 1.5 to 2 hours and is carried out under general anaesthesia.
How is the procedure performed ?
The operation is generally performed by keyhole (laparoscopic) surgery. The surgeon will make four to five small cuts in your abdomen wall. The surgeon will tighten the opening (hiatus) and wrap the top part of the stomach around the lower part of your gullet as in picture to form a new valve that will stop acid from pushing back up into the foodpipe. There are different types of wraps that can be formed around the lower gullet; your surgeon will decide on the most appropriate type for you. The operation usually takes about 1.5 – 2 hours. In a small number of cases, the operation cannot be completed by keyhole surgery. In this situation, the keyhole operation is ‘converted’ to an open operation. The stitches on the skin are dissolvable.

Are there any potential side-effects or complications after surgery?
Anti-reflux surgery is as safe as most other types of routine surgery such as gallbladder removal or inguinal hernia repair. Any type of surgery, however, can involve some potential risks which in this procedure include bleeding, infection, damage to any of the organs in the region such as stomach or oesophagus.
There are certain side-effects specific to fundoplication like
• Belching
• Bloating
• Flatulence
These side effects should resolve over the course of a few months.
What is the recovery like after surgery?
- By evening patients are able to walk and can have fluids by mouth.
- Most of patients go home after 24 hours, however some may have to stay for a day extra depending on recovery and social circumstances.
- You can return to non-strenuous activity (going to office) within a couple of days, but you must avoid strenuous activity for six weeks.
- You should not drive for 2 weeks however you can travel by cab.


What is the dietary advice following surgery?
- There are restrictions to food intake for the first few weeks after the operation.
- You should only drink water for the rest of the day after the operation.
- Our dietician will formulate a diet plan for next four weeks depending on your social and religious beliefs.
- Some patients become constipated and need to take laxatives if their bowels have not opened.
- If you have any difficulties with certain foods discuss this with your consultant or dietitian. At your 4 week follow-up appointment with your consultant/ dietician you may start a normal diet.
Cost of Gastric Reflux Surgery
- Bed category
- Type of surgery
- Open or laparoscopic repair
- Choice of hospital
- Preexisting medical conditions such as diabetes, angina which may prolong your hospital stay or need critical monitoring. Following your first meeting with the doctor, we would be able to give you an approximate estimate.