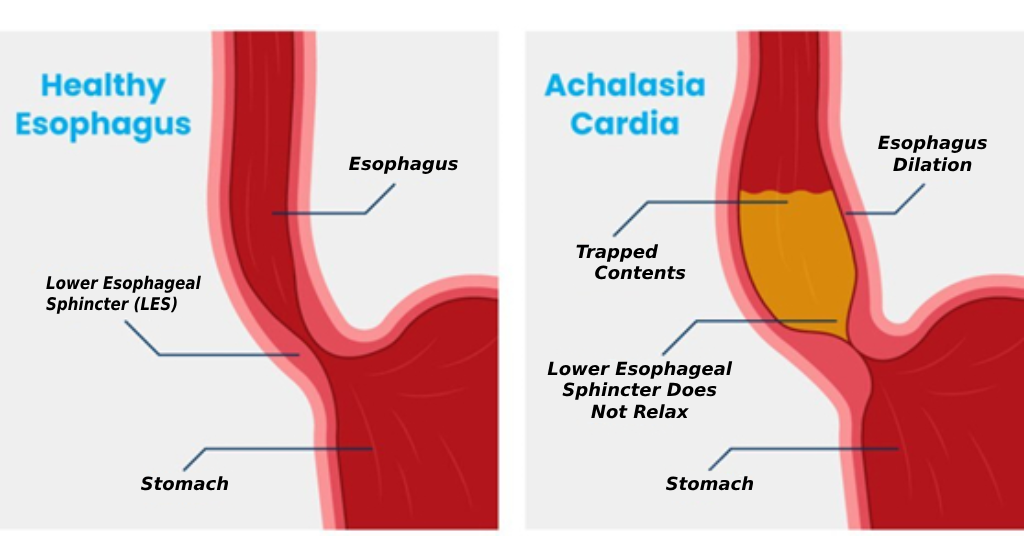
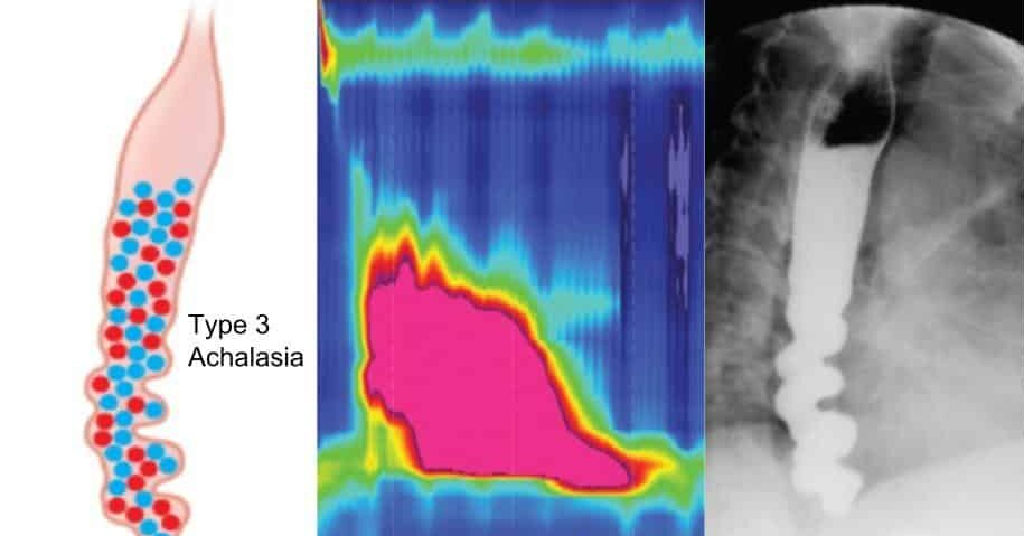
Oesophagus or food pipe (अन्ननलिका) is a muscular tube which connects the mouth to the stomach. When food or drink is swallowed, muscles in the food pipe contract and relax to push food into the stomach. This is known as peristalsis. At the bottom of the oesophagus and near its junction with the stomach is a valve called the lower oesophageal sphincter (LES).
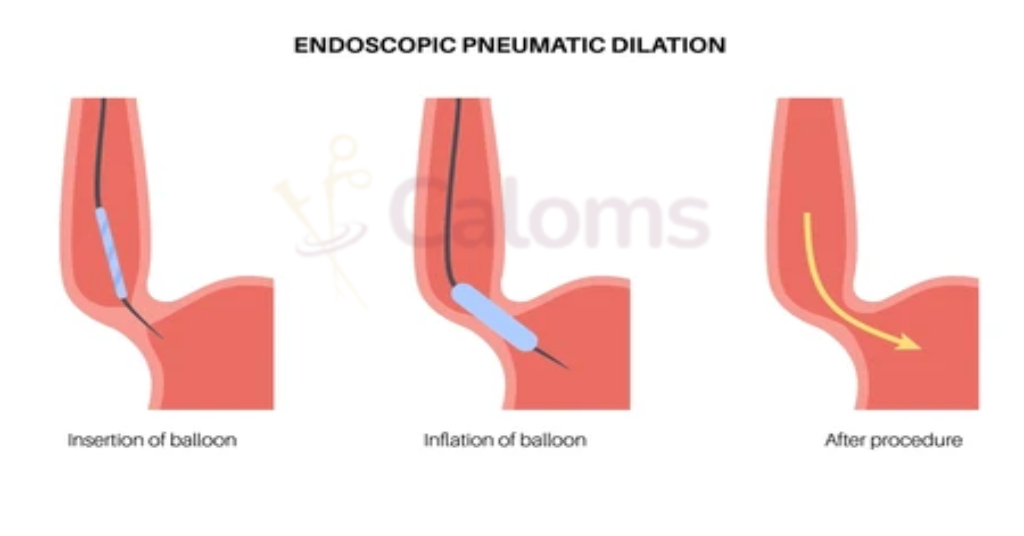
When you swallow, the lower oesophageal sphincter opens to allow food and drink into the stomach. In achalasia, the muscles in the oesophagus do not contract correctly, and the ring of muscle at the bottom end (LES) can fail to open properly, or does not open at all. As a result, the oesophagus loses its ability to transfer food and drink into the stomach. This is a problem which affects the nerves and muscles of the oesophagus and LES.